Ah, EMTALA! The revered ‘Emergency Medical Treatment and Active Labor Act!’ It’s one of those things which is like a nursery rhyme to emergency medicine folks like me. We’ve heard about it from the infancy of our training. ‘And then the bad doctor sent the poor lady to another hospital because she couldn’t pay! And the King came and crucified him for doing it!’ The end.
EMTALA, for the uninitiated, is a federal law which ensures that we don’t turn people away from the ER because of finances, and also keeps us from transferring people to other hospitals without that hospital’s agreement. It also exists to guarantee that we stabilize them as much as possible before they go.
I’ve said before, and always will, it was a good idea. But like many laws, it was subject to the law of unintended consequences. For instance, being forced to see lots and lots of people (who may not really be that sick), and do it for free, has huffed, and puffed and blown the hospital and trauma center down on too many occasions. But that’s not my point here.
My point is that when EMTALA forms meet electronic medical records, chaos can ensue.
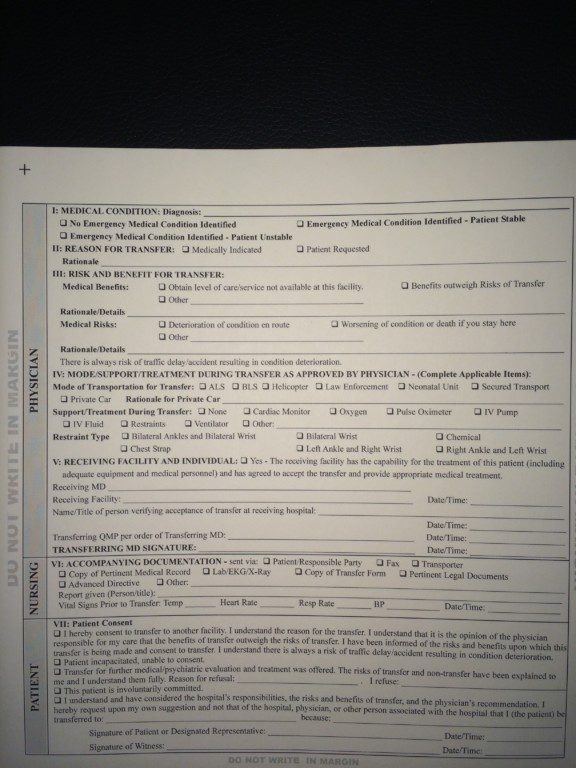
Allow me to illustrate: This is a standard EMTALA form. Check, check, check, sign. It takes a busy physician less than a minute, and the nurses a few more since they have to call the other hospital and record times, etc. This has worked well for a very, very long time.
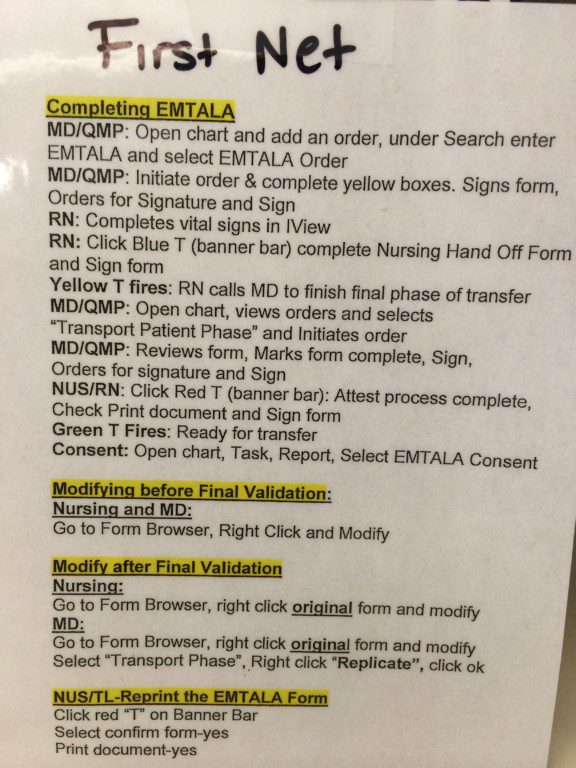
Enter EMR. This is the procedure for doing an EMTALA form at Tiny Memorial Hospital, which has been enchanted by the dark Lord Cerner. Mind you, I’m sure the ‘powers that be’ feel that this is a perfectly wonderful way to do the form. Indeed, it captures lots of information and stores it in the system. But two facts remain: first, the people who designed the system generally work at Large Urban Hospital, which owns Tiny Memorial. They don’t transfer things out very often. They receive things. Second, most of the patients being transferred are going within the system. All the data is on the EMR, and it isn’t as if they’re going to some strange facility far, far away.
This, children, is the EMR based procedure (on a cheat sheet developed by a frustrated and confused provider):
Not long ago my team worked a cardiac arrest at Tiny Memorial, with a successful return of cardiac activity. Given our size and staffing, it took pretty much all of the staff available and nothing moved for a while. A helicopter whisked our patient away.
Of all the things we did; drag her out of the car, do CPR, start IV’s, intubate, talk with family, chart, arrange transfer, nothing was as complicated or frustrating as this process to complete the EMTALA form. In the end, I still got it wrong somehow.
Mind you, I never violated the spirit of the law in any way. She was treated, stabilized (to the extent of our ability) and sent away to a receiving hospital with the capacity to care for her.
I don’t want to impugn the motives of those who developed this. I’m sure they were trying their best. But if you don’t use it, you can’t see how hard it is. And you also can’t see how much time it takes in a place with limited resources and staff.
So please, folks, let’s use technology to simplify, not make things more complicated! And let’s remember that charting isn’t the same as doing the right thing. And sometimes, doing the right thing isn’t perfectly reflected in the chart.
But paper or electrons, it’s still the right thing. And that’s what EMTALA is about.
Hi Ed. I have much enjoyed reading you throughout my 32 year (now retired) ER run. I am currently penning my memories and teachings, “the411onthe911”, and continue to be inspired by your vision and writing. I am coming to appreciate the difficult task of writing a book, and compliment you on the tenacity it obviously takes. However, we are tenacious people, us ER folks. I would love to stay in touch with you as I complete my mission. Upon my retirement from the floor, I have developed a tattoo removal practice, Physicians Advanced Laser Center, zaptheink.com, as well as my… Read more »
{"id":null,"mode":"form","open_style":"in_place","currency_code":"USD","currency_symbol":"$","currency_type":"decimal","blank_flag_url":"https:\/\/edwinleap.com\/wp-content\/plugins\/tip-jar-wp\/\/assets\/images\/flags\/blank.gif","flag_sprite_url":"https:\/\/edwinleap.com\/wp-content\/plugins\/tip-jar-wp\/\/assets\/images\/flags\/flags.png","default_amount":100,"top_media_type":"none","featured_image_url":false,"featured_embed":"","header_media":null,"file_download_attachment_data":null,"recurring_options_enabled":true,"recurring_options":{"never":{"selected":true,"after_output":"One time only"},"weekly":{"selected":false,"after_output":"Every week"},"monthly":{"selected":false,"after_output":"Every month"},"yearly":{"selected":false,"after_output":"Every year"}},"strings":{"current_user_email":"","current_user_name":"","link_text":"Leave a tip","complete_payment_button_error_text":"Check info and try again","payment_verb":"Pay","payment_request_label":"EdwinLeap.com","form_has_an_error":"Please check and fix the errors above","general_server_error":"Something isn't working right at the moment. Please try again.","form_title":"EdwinLeap.com","form_subtitle":"If you enjoy the content you read here, please consider dropping something in the tip jar!","currency_search_text":"Country or Currency here","other_payment_option":"Other payment option","manage_payments_button_text":"Manage your payments","thank_you_message":"Thank you so much! I appreciate the tip!","payment_confirmation_title":"EdwinLeap.com","receipt_title":"Your Receipt","print_receipt":"Print Receipt","email_receipt":"Email Receipt","email_receipt_sending":"Sending receipt...","email_receipt_success":"Email receipt successfully sent","email_receipt_failed":"Email receipt failed to send. Please try again.","receipt_payee":"Paid to","receipt_statement_descriptor":"This will show up on your statement as","receipt_date":"Date","receipt_transaction_id":"Transaction ID","receipt_transaction_amount":"Amount","refund_payer":"Refund from","login":"Log in to manage your payments","manage_payments":"Manage Payments","transactions_title":"Your Transactions","transaction_title":"Transaction Receipt","transaction_period":"Plan Period","arrangements_title":"Your Plans","arrangement_title":"Manage Plan","arrangement_details":"Plan Details","arrangement_id_title":"Plan ID","arrangement_payment_method_title":"Payment Method","arrangement_amount_title":"Plan Amount","arrangement_renewal_title":"Next renewal date","arrangement_action_cancel":"Cancel Plan","arrangement_action_cant_cancel":"Cancelling is currently not available.","arrangement_action_cancel_double":"Are you sure you'd like to cancel?","arrangement_cancelling":"Cancelling Plan...","arrangement_cancelled":"Plan Cancelled","arrangement_failed_to_cancel":"Failed to cancel plan","back_to_plans":"\u2190 Back to Plans","update_payment_method_verb":"Update","sca_auth_description":"Your have a pending renewal payment which requires authorization.","sca_auth_verb":"Authorize renewal payment","sca_authing_verb":"Authorizing payment","sca_authed_verb":"Payment successfully authorized!","sca_auth_failed":"Unable to authorize! Please try again.","login_button_text":"Log in","login_form_has_an_error":"Please check and fix the errors above","uppercase_search":"Search","lowercase_search":"search","uppercase_page":"Page","lowercase_page":"page","uppercase_items":"Items","lowercase_items":"items","uppercase_per":"Per","lowercase_per":"per","uppercase_of":"Of","lowercase_of":"of","back":"Back to plans","zip_code_placeholder":"Zip\/Postal Code","download_file_button_text":"Download File","input_field_instructions":{"tip_amount":{"placeholder_text":"How much would you like to tip?","initial":{"instruction_type":"normal","instruction_message":"How much would you like to tip? Choose any currency."},"empty":{"instruction_type":"error","instruction_message":"How much would you like to tip? Choose any currency."},"invalid_curency":{"instruction_type":"error","instruction_message":"Please choose a valid currency."}},"recurring":{"placeholder_text":"Recurring","initial":{"instruction_type":"normal","instruction_message":"How often would you like to give this?"},"success":{"instruction_type":"success","instruction_message":"How often would you like to give this?"},"empty":{"instruction_type":"error","instruction_message":"How often would you like to give this?"}},"name":{"placeholder_text":"Name on Credit Card","initial":{"instruction_type":"normal","instruction_message":"Enter the name on your card."},"success":{"instruction_type":"success","instruction_message":"Enter the name on your card."},"empty":{"instruction_type":"error","instruction_message":"Please enter the name on your card."}},"privacy_policy":{"terms_title":"Terms and conditions","terms_body":null,"terms_show_text":"View Terms","terms_hide_text":"Hide Terms","initial":{"instruction_type":"normal","instruction_message":"I agree to the terms."},"unchecked":{"instruction_type":"error","instruction_message":"Please agree to the terms."},"checked":{"instruction_type":"success","instruction_message":"I agree to the terms."}},"email":{"placeholder_text":"Your email address","initial":{"instruction_type":"normal","instruction_message":"Enter your email address"},"success":{"instruction_type":"success","instruction_message":"Enter your email address"},"blank":{"instruction_type":"error","instruction_message":"Enter your email address"},"not_an_email_address":{"instruction_type":"error","instruction_message":"Make sure you have entered a valid email address"}},"note_with_tip":{"placeholder_text":"Your note here...","initial":{"instruction_type":"normal","instruction_message":"Attach a note to your tip (optional)"},"empty":{"instruction_type":"normal","instruction_message":"Attach a note to your tip (optional)"},"not_empty_initial":{"instruction_type":"normal","instruction_message":"Attach a note to your tip (optional)"},"saving":{"instruction_type":"normal","instruction_message":"Saving note..."},"success":{"instruction_type":"success","instruction_message":"Note successfully saved!"},"error":{"instruction_type":"error","instruction_message":"Unable to save note note at this time. Please try again."}},"email_for_login_code":{"placeholder_text":"Your email address","initial":{"instruction_type":"normal","instruction_message":"Enter your email to log in."},"success":{"instruction_type":"success","instruction_message":"Enter your email to log in."},"blank":{"instruction_type":"error","instruction_message":"Enter your email to log in."},"empty":{"instruction_type":"error","instruction_message":"Enter your email to log in."}},"login_code":{"initial":{"instruction_type":"normal","instruction_message":"Check your email and enter the login code."},"success":{"instruction_type":"success","instruction_message":"Check your email and enter the login code."},"blank":{"instruction_type":"error","instruction_message":"Check your email and enter the login code."},"empty":{"instruction_type":"error","instruction_message":"Check your email and enter the login code."}},"stripe_all_in_one":{"initial":{"instruction_type":"normal","instruction_message":"Enter your credit card details here."},"empty":{"instruction_type":"error","instruction_message":"Enter your credit card details here."},"success":{"instruction_type":"normal","instruction_message":"Enter your credit card details here."},"invalid_number":{"instruction_type":"error","instruction_message":"The card number is not a valid credit card number."},"invalid_expiry_month":{"instruction_type":"error","instruction_message":"The card's expiration month is invalid."},"invalid_expiry_year":{"instruction_type":"error","instruction_message":"The card's expiration year is invalid."},"invalid_cvc":{"instruction_type":"error","instruction_message":"The card's security code is invalid."},"incorrect_number":{"instruction_type":"error","instruction_message":"The card number is incorrect."},"incomplete_number":{"instruction_type":"error","instruction_message":"The card number is incomplete."},"incomplete_cvc":{"instruction_type":"error","instruction_message":"The card's security code is incomplete."},"incomplete_expiry":{"instruction_type":"error","instruction_message":"The card's expiration date is incomplete."},"incomplete_zip":{"instruction_type":"error","instruction_message":"The card's zip code is incomplete."},"expired_card":{"instruction_type":"error","instruction_message":"The card has expired."},"incorrect_cvc":{"instruction_type":"error","instruction_message":"The card's security code is incorrect."},"incorrect_zip":{"instruction_type":"error","instruction_message":"The card's zip code failed validation."},"invalid_expiry_year_past":{"instruction_type":"error","instruction_message":"The card's expiration year is in the past"},"card_declined":{"instruction_type":"error","instruction_message":"The card was declined."},"missing":{"instruction_type":"error","instruction_message":"There is no card on a customer that is being charged."},"processing_error":{"instruction_type":"error","instruction_message":"An error occurred while processing the card."},"invalid_request_error":{"instruction_type":"error","instruction_message":"Unable to process this payment, please try again or use alternative method."},"invalid_sofort_country":{"instruction_type":"error","instruction_message":"The billing country is not accepted by SOFORT. Please try another country."}}}},"fetched_oembed_html":false}

Hi Ed. I have much enjoyed reading you throughout my 32 year (now retired) ER run. I am currently penning my memories and teachings, “the411onthe911”, and continue to be inspired by your vision and writing. I am coming to appreciate the difficult task of writing a book, and compliment you on the tenacity it obviously takes. However, we are tenacious people, us ER folks. I would love to stay in touch with you as I complete my mission. Upon my retirement from the floor, I have developed a tattoo removal practice, Physicians Advanced Laser Center, zaptheink.com, as well as my… Read more »