

Unless you’ve been living under a rock, you’re well aware that the United States is in the grip of a really big epidemic of opioid abuse. The epicenter of much of this has been my beloved Appalachia. My home-town, Huntington, WV, might as well be re-named ‘Oxycontin,’ or maybe ‘Heroinville.’ It’s ugly.
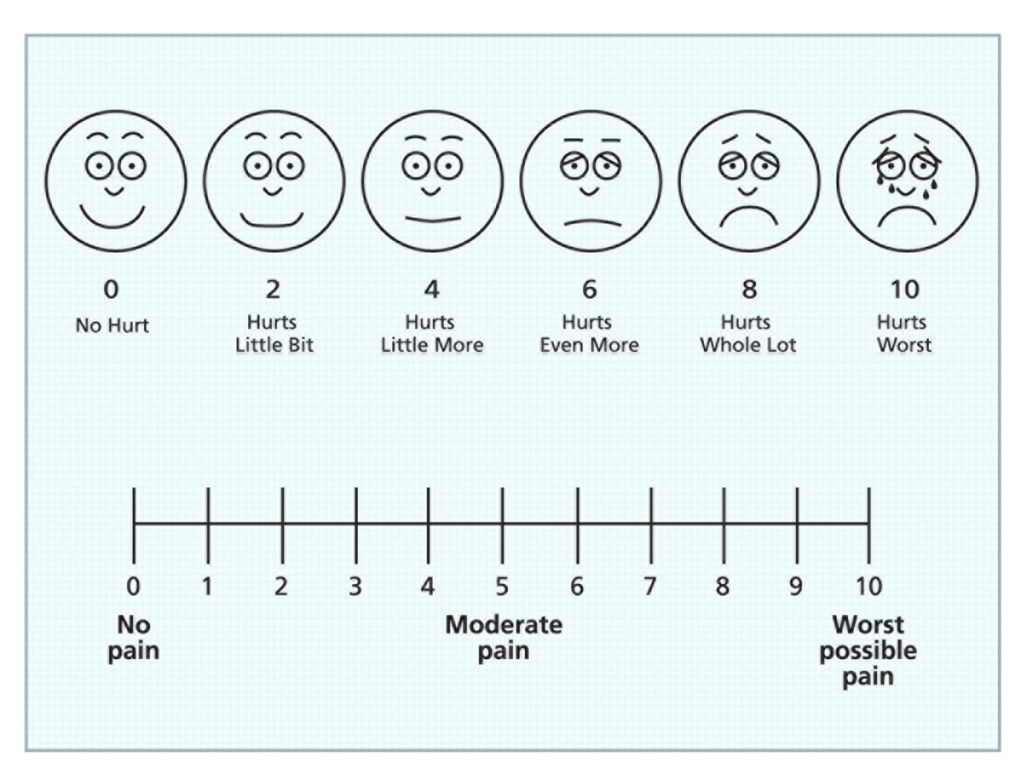
Enormous amounts of ink have been spilled on this topic, and I don’t intend to explain the genesis of it in detail. In short, however, about 20 years ago some doctors thought we weren’t being kind enough in our treatment of pain. Some articles were published to draw attention to this theory. We started using the pain scale. 0 = no pain, 10 = the worst pain ever.
Around the same time administrators discovered the customer/patient satisfaction score. Taken together, physicians and nurses were pressured by 1) academic peers and medical directors as well as 2) administrators, to give more pain medication.
So, to recap mathematically:
Pain scale x Satisfaction score = better reimbursement + death
Recently, smart people have discovered that a lot of what we were told to do in clinical practice was probably (to put it delicately) utterly stupid and ultimately deadly. Having said that, not all of the drug abuse in the country is because doctors gave out too many pills (although pill-mills are obviously a problem).
Some of it, in particular the heroin and fentanyl nightmare, has to do with bad decisions, experimentation and the high marketability of those drugs. Enormous amounts of those drugs are manufactured in other countries and shipped here (obviously illegally). Money talks, as it were.
The problem is, research suggests that patients of doctors with very high satisfaction scores often do poorly. Think of your kids. How do they turn out if you give them whatever they ask? Not usually very well. Often quite badly. Ditto for patient care. Nobody should get a CT scan or antibiotic just because they want it. Nor should they get narcotics just because they scream ‘it’s a ten!’ Or because they ask to talk to the patient advocate or administrator.
The further problem is that administrators (and government) seem to be lagging behind science. (Not that doctors don’t also; can’t throw too many stones in the glass house.) But they get all worried when people complain that their pain wasn’t treated. And indeed, in many insurance payment schemes, pain management is really important. Don’t treat pain? Don’t get reimbused well.
Ultimately, however, this national obsession with pain relief has landed squarely in the emergency departments of the land. I work in a mid-volume emergency department in a community hospital. And I’ll recap a few pain complaints that I have seen which illustrate the problem:
‘I had dental surgery and my oral surgeon said if my pain was worse I should go to the ER.’ My pain? It’s about a 9/10.’ (Texting and laughing.)
‘I had a car wreck a month ago and broke some ribs. I missed my follow-up appointment but I need more pain medicine. My pain is a 10/10.
‘I fell down and hurt my knee yesterday. (Xrays negative, mild swelling.) Tylenol and Motrin are like taking candy. I need something stronger.’
‘I go to the Methadone clinic but I didn’t get there today and I need pain control.’]
‘I’ve had sinus pressure for a few days. No, I didn’t take anything for it. I came here!’
‘I hurt all over, and I’m hot and cold and sweating, and my wife says I have a fever, but I think I’m dying.’ (Did you take anything, he asked, knowing the answer ahead of time?) ‘I didn’t take anything. I just came here.’
‘This cough is driving me crazy. Can’t you give me something stronger for my pain?’ Yep, an inhaler so you won’t cough. And here’s a thought. Stop smoking!
‘My 7-year-old daughter skinned her knee a few days ago and says that Tylenol and Motrin don’t help at all. Her pain is an 8/10.’ A child with a minor injury understands to rate her pain higher…
‘I just started a job as a brick-mason and my back is sore. Can I get something stronger for the pain?’
‘I have migraines. My pain is a 15/10 and Imitrex does not help. The only thing that helps is Dilaudid. Morphine is like water…’ (????)
‘Well if my wrist isn’t broken from the fall, Doctor, how come it hurst so much! I mean, it’s a 10/10!’ (Uh, it’s bruised?)
‘My family doctor doesn’t give narcotics. His office says I should go to the ER.’
‘My pain specialist is out of the country and his office says I should go to the ER.’
The list is exhaustive. Ask your nurse and doctor friends; especially those who work in emergency medicine. Ask them about the pain scale and watch them roll their eyes.
We’ve turned pain into a religion; worse, into a kind of physical victimization in which the victim of the pain is always right. And is always entitled. In the process, we have allowed people to forget that pain is important and normal. That it is necessary for our safety. That it probably helps healing; a body that doesn’t know there’s a problem doesn’t heal as well.
And we’ve created far too many people whose entire lives are predicated on a drowsly euphoria spent sitting on the couch or in the bed, while other people provide for them and care for them.
In addition, the constant requests for pain meds can distract us from those in genuine pain, and who really, truly need the ‘good stuff.’ The fractures, cancers, sickle-cell, and other patients who need urgent relief.
This is immoral. It’s bad, bad, bad for our patients. But it’s also terrible for our hospitals; in particulary my beloved emergency department. Because it means that around the clock, even as we try to make decisions that will hopefully save lives and prevent permanent harm, we are tasked with responding to every whim of the pain-scale.
All day, and in particular all night, our societal pain obsession has been shifted onto the backs of physicians and nurses in the ER. There is seldom a break from this. And because federal law prohibits financial screening in the ER, many of our more nefarious and manipulative ‘customers’ know that if the pain clinic expects cash, at least the ER doesn’t. If the surgeon wants money to see you in follow-up, you can hoof it to the nearest ER and get pain meds (if you’re annoying enough) and maybe a sandwich or a ride home. And with all due respect, our Medicaid population knows the same thing. So a 3 AM visit for a minor complaint (with pain thrown in as a side) might get some narcotics; and doesn’t cost anything personally.
This leaves staff members exhausted, bitter and burned out. More so when administrators habitually take the side of the ‘customer’ against the already overwhelmed staff.
The bottom line is we’re hurting people. Patients and professionals alike.
And it turns out, this is so pervasive that even the dogs have pain scales. My wife and I cracked up when we saw this in the vet’s office. I mean, pain relief is fine for dogs (it’s mostly NSAIDs). But a visual analog pain scale for dogs?
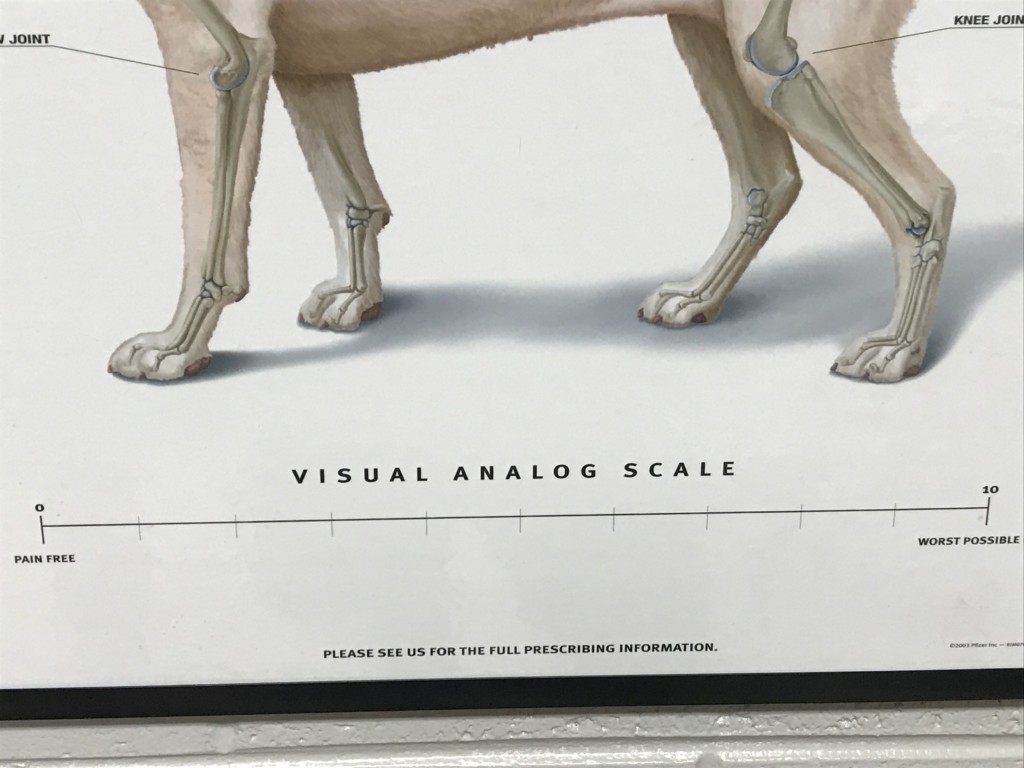
‘Lassie! Bark once for each pain scale level! What’s that? 20 barks? What are you a pure-bred Lab? It only goes to ten. You’re a drug seeker and you have a problem…Wait, is that my prescription pad? Go home, you’re stoned…’
America, not all pain needs to be suppressed and most pain doesn’t require an ER visit. Many people do need pain relief, and this frantic desire to treat every little ache and discomfort makes it harder for us to threat the ones really hurting.
And sometimes, when it comes to your pain scale, you’re just stupid.

{kind=link}
After a short hospitalization for a blocked small bowel, the discharging physician finally asked me how much pain medicine I needed. I thought, that was the smartest and best-timed question I had heard during my stay. Don’t fire that doc; he’s a keeper.
[…] Even dogs get pain scales. […]
Thank you for the link! I’m honored to be included.
While I personally stay away from heavy pain meds in all but extreme circumstances (shoulder replacement after trauma and then only for 2 weeks), I wouldn’t presume to judge someone else’s pain. Yeah, I have seen people in doctor’s offices who have been trying to trick them into this and heard about more from pharmacist friends. I have also known of people who have been denied needed meds. And the “experts” use those pain scales which are completely useless. Is a gunshot wound more painful than childbirth. Damn if I know since I have never experienced either. And how do… Read more »
Unless you have experienced a migraine you have no legitimate basis for deciding what pain a person is suffering, and suffering is the right word for migraine. I have dealt with migraine for years and it appears it will be my chore to do so until the Lord lets me go home. At the time of his choosing, not mine. I don’t like pain meds. Most have side effects I prefer to live without. There are times though when the combination of severe pain, nausea, and extreme sensitivity to light and sound make me willing to take a pain Med… Read more »
Actually I’ve had some bad headaches and I often have often given narcotics for severe migraines. But I think, after 24 years of medical practice, I probably have a litle insight into things that are reasonable indications for strong pain meds and things that aren’t. I just think that our cultural expectations for pain relief have gotten way off track.
I stand corrected. Your article came across to me as classifying all migraine sufferers who come into the ED as fakes who want narcotics, and not that any have legitimate complaints. Unfortunately, those who just want the drugs for a high or whatever they get from it give those who actually need a significant pain reliever a bad reputation as fakes, keeping the legit patients from getting the relief they could use. Perhaps the headache I had when I read the article helped me read you incorrectly.
I apologize.
G M
No problem! And you make a good point. We have to carefully, compassionately, separate the wheat from the chaff…some docs refuse to use any narcotics for migraine, and there are good alternatives. But I never rule out their use.